A popular phrase in tumor immunology is that an effective intratumoral intervention can “turn the tumor into a vaccine.” The phrase is useful because it points at a real mechanistic aspiration: use the tumor itself as the antigen source, then supply the right inflammatory context so the immune system generates tumor-specific T cells capable of trafficking and killing disease elsewhere. But the slogan can also conceal the difficulty. Vaccination is not simply “antigen + immune stimulation.” It is antigen, adjuvant, and architecture, all aligned in time.
Thinking in those three terms is a disciplined way to evaluate intratumoral immunotherapy without drifting into hype.
1) Antigen: the tumor is a library, not a single target
Traditional vaccines usually present a defined antigen, or a small set of antigens, chosen for stability and immunogenicity. Tumors are different. They express thousands of proteins, many shared with normal tissue, and only a subset are relevant targets. Even when “neoantigens” exist (tumor-specific mutations that can generate new peptides), not all are presented effectively, and not all elicit strong T cell recognition.
So the tumor is not a clean antigen. It is a library with noisy labeling.
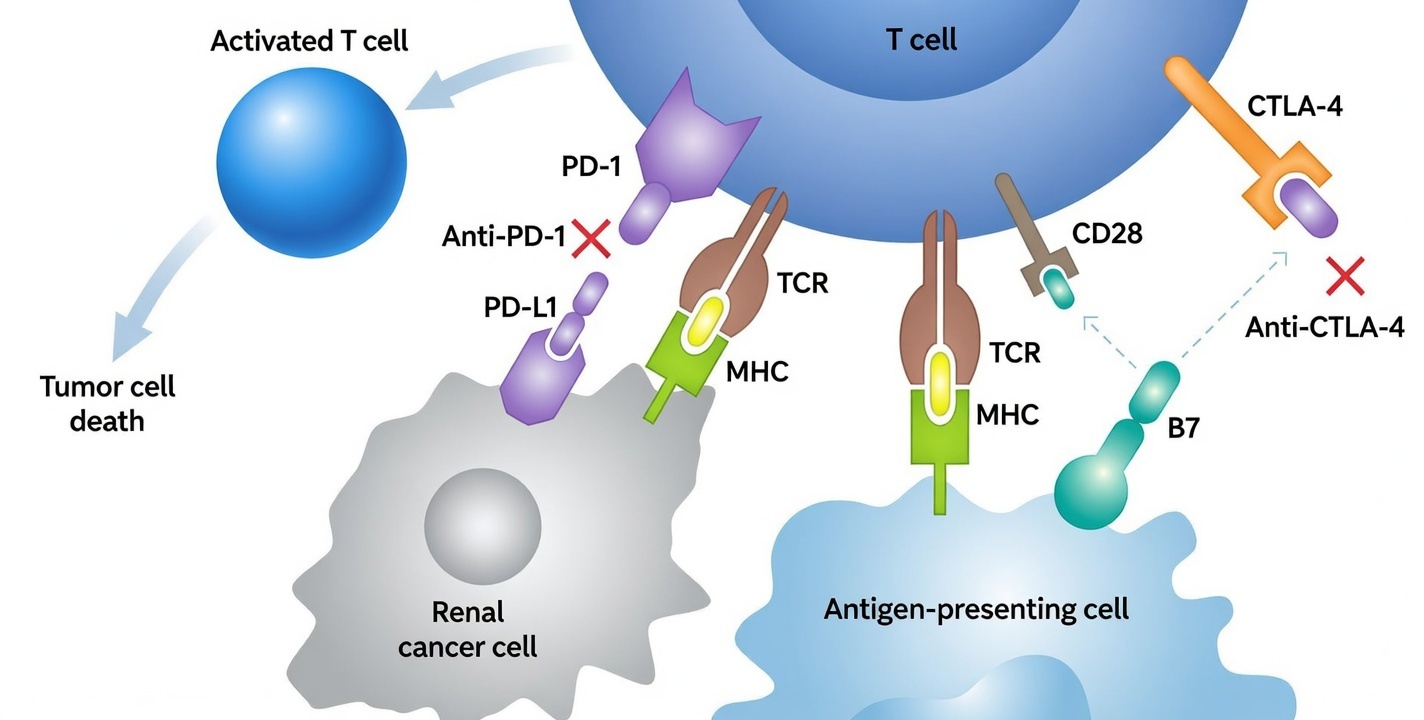
A local therapy that causes tumor cell death may increase antigen availability, but availability alone does not guarantee productive immunity. Antigens must be captured by antigen-presenting cells (especially dendritic cells), processed, and displayed on MHC molecules in a way that matches T cell receptors. The immune system is strict: it responds not to “tumor-ness,” but to precise peptide–MHC encounters, in the right activation context.
This is why “more antigen” can still fail. If the presentation is poor, or if the immune context is suppressive, antigen exposure can even reinforce tolerance-like states.
2) Adjuvant: inflammation must be instructive, not merely intense
In vaccinology, an adjuvant is not simply a substance that causes inflammation. It is a signal that tells the immune system what kind of response to build. Different innate sensing pathways bias toward different downstream programs: cytotoxic T cell responses, antibody-driven immunity, or regulatory damping. Tumors exploit this by creating chronic low-grade inflammation that recruits suppressive myeloid cells and blunts effective priming.
A key concept here is immunogenic cell death: some forms of cell death release “danger signals” that activate antigen-presenting cells, while others are comparatively silent. Intratumoral therapy aims to generate cell death plus the right innate cues so dendritic cells mature rather than merely clean up debris.
But the immune system is not a simple amplifier. Overstimulation, prolonged stimulation, or poorly targeted stimulation can recruit the wrong players: regulatory T cells, suppressive macrophages, exhausted effector T cells. So the challenge is to deliver inflammation that is informational, not just loud.
This is one reason controlled local delivery platforms matter: they can shape the magnitude and duration of innate activation, influencing whether the immune response is organized or chaotic.
3) Architecture: the tumor microenvironment is an immune filter
Even if antigen is abundant and adjuvant signals are present, tumors can still remain resistant because the tissue is physically and functionally organized to block immune effectors.
Architecture has multiple layers:
- Physical barriers: dense extracellular matrix can prevent immune cell penetration.
- Vascular barriers: abnormal vessels create irregular trafficking and hypoxia.
- Cellular zoning: suppressive myeloid cells may occupy perivascular spaces and exclude cytotoxic T cells.
- Signal gradients: cytokines and metabolites form microdomains that bias immune fate locally.
Architecture is why systemic checkpoint blockade can work brilliantly in some tumors and poorly in others. It is also why intratumoral strategies are attractive: they let one intervene at the level of tissue logic, not only molecular logic.
However, architecture is also why intratumoral therapy is not trivially repeatable. Two tumors in the same patient can have different architecture; two regions in the same tumor can behave differently. So the “vaccine” analogy is not one product replicated across bodies, but a process attempting to force an immune system to learn from a messy and evolving tissue.
The bridge to systemic impact: priming, trafficking, recognition
If the goal is systemic control (including abscopal-like outcomes), local immunotherapy must accomplish at least three downstream feats:
- Priming: generate tumor-reactive T cells in sufficient quantity and quality.
- Trafficking: enable these cells to reach distant lesions, survive, and infiltrate.
- Recognition: ensure the distant tumor presents the same relevant antigens and is not fully shielded by local suppression.
Intratumoral interventions can strongly influence priming and the “meaning” of antigen exposure. Trafficking and recognition often require additional factors: systemic immune tone, vascular access, and overcoming inhibitory pathways at distant sites.
This is why combination strategies are common in the field, and why careful clinical design matters more than slogans.
Conclusion: a sober promise
The intellectually honest promise of intratumoral immunotherapy is not that a tumor becomes a vaccine automatically. It is that local therapy can be engineered to create a high-quality immune lesson—one that makes tumor antigens legible, presented in a mature and activating context, within tissue architecture that permits effector function.
Put differently: the goal is not to inject hope into a tumor. The goal is to design the conditions under which the immune system can do what it already evolved to do—recognize, learn, remember, and eliminate—despite the tumor’s best attempts to scramble the lesson.
That’s a hard problem. It’s also the kind of problem that, when solved even partially, changes the shape of what oncology can be.