Intratumoral therapy is often described as a change in delivery route: instead of dosing a drug systemically and hoping adequate exposure reaches the tumor, clinicians place therapy directly into malignant tissue. That description is accurate but incomplete. The deeper idea is that intratumoral immunotherapy treats cancer as a systems problem—one governed by spatial constraints, time-dependent signaling, and an evolving microenvironment that determines whether immune recognition becomes durable or dissipates.
In solid tumors, the immune system rarely fails for a single reason. Failure is typically emergent: physical architecture limits immune cell entry; cytokine gradients and stromal remodeling shape local behavior; antigen presentation and T cell priming may occur, but are suppressed or misdirected by regulatory networks. As a result, the most consequential variable may not be the identity of a molecule in isolation, but the context in which immune stimuli occur. Intratumoral approaches are compelling because they allow direct intervention in that context.
The tumor microenvironment is an engineered obstacle
Solid tumors are not merely collections of transformed cells. They are complex tissues comprising malignant cells, fibroblasts, endothelial cells, macrophages, dendritic cells, extracellular matrix, and soluble mediators. This network can become immunologically “cold” through several convergent mechanisms:
- Physical exclusion: dense extracellular matrix and aberrant vasculature can limit immune infiltration and generate irregular perfusion.
- Metabolic stress: hypoxia and nutrient competition bias immune cells toward dysfunctional phenotypes.
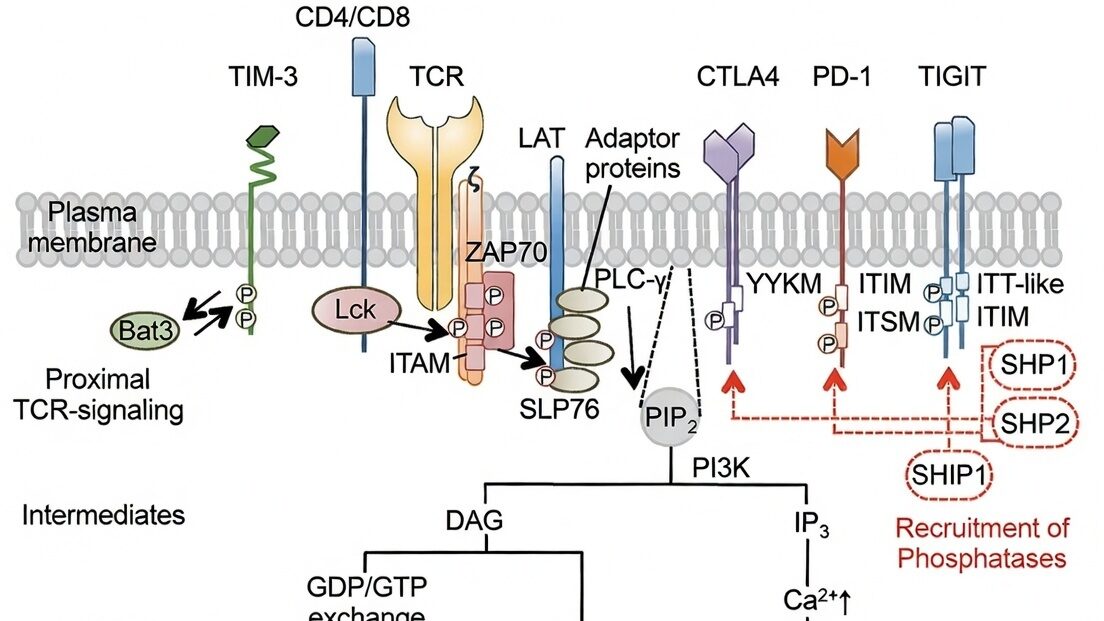
- Active suppression: tumor-associated macrophages and regulatory T cells can dampen cytotoxic responses; inhibitory signaling pathways maintain tolerance-like states.
These features are not static. They shift with tumor growth, therapy exposure, and immune adaptation. A purely systemic immune modulator must contend with these local barriers without being able to directly reorganize them. By contrast, intratumoral dosing offers a way to place an immune perturbation precisely within the microenvironment’s “control room.”
Space: distribution is a biological variable, not a pharmacokinetic footnote
In systemic pharmacology, distribution is often treated as a quantitative constraint: insufficient exposure in tumor tissue limits efficacy. In intratumoral settings, distribution becomes a qualitative variable that can shape immune outcome.
Local deposition determines whether immune stimulation is focal or diffuse, whether antigen-presenting cells encounter relevant signals, and whether gradients of cytokines or danger signals support coordinated activation. If local therapy disperses too quickly or unevenly, the immune system may receive fragmented cues—insufficient to produce robust priming or memory. Conversely, a controlled spatial exposure can promote a coherent inflammatory “scene” in which antigen release, innate activation, and adaptive priming occur in synchrony.
This is one reason materials science and formulation matter in intratumoral design.
A delivery system that increases local retention or moderates spread can help transform a single injection into a structured immune event rather than a transient chemical pulse.
Time: immune activation requires persistence, but not indiscriminate persistence
Immune responses unfold on timescales that differ from small-molecule pharmacokinetics. Innate sensing and antigen uptake can occur within hours, but dendritic cell maturation, lymph node trafficking, T cell priming, clonal expansion, and differentiation into memory phenotypes occur over days to weeks.
An intervention that disappears too quickly may initiate inflammation without enabling the downstream sequence required for durable adaptive immunity.
However, persistence is not inherently beneficial. Chronic stimulation can lead to exhaustion, tolerance, or compensatory suppression. The therapeutic goal is therefore not maximal duration but biologically matched duration: enough sustained local signaling to support antigen presentation and priming, while avoiding prolonged nonspecific inflammation that recruits suppressive cell types or damages healthy tissue.
This logic again points toward engineered release profiles—approaches that shape exposure to align with immune kinetics rather than purely with chemical stability.
From local intervention to systemic consequence
The phrase “abscopal effect” refers to distant tumor regression associated with localized treatment. Mechanistically, an abscopal-like outcome can be framed as a sequence:
- Local tumor disruption generates antigen availability and danger-associated signals.
- Antigen-presenting cells process tumor antigens in an activated context.
- Adaptive priming expands tumor-reactive T cell populations.
- Trafficking and infiltration enable these effector cells to reach distant lesions.
- Recognition and killing proceed if inhibitory mechanisms are overcome.
Each step is contingent. Tumor antigens must be presented with appropriate costimulation; primed cells must survive and traffic; distant tumors must be penetrable and not fully immunologically suppressed. Intratumoral strategies are attractive because they can strongly influence steps 1 and 2, and partially influence step 3 by controlling the quality of the initiating event. Whether steps 4 and 5 occur depends on broader systemic conditions, and often requires combination strategies or careful patient selection.
A rigorous view of “platform” in intratumoral therapy
A platform in this setting should be understood as a repeatable way to engineer space–time–signal relationships in tumors. The “payload” may vary—immune agonists, antibodies, cytokines, or other agents—but the enabling hypothesis remains: properly structured local exposure can convert a tumor from an immune-evasive tissue into an immunologically legible one.
Crucially, this is not a claim that intratumoral delivery is universally superior. Some tumors are inaccessible or unsafe to inject; some lesions are too diffuse; some disease biology may require systemic exposure. The academic argument is narrower and more defensible: for selected solid tumors, local control over microenvironmental conditions offers an unusually direct lever on immune behavior.
Conclusion
Intratumoral immunotherapy is best interpreted not as a procedural convenience but as a scientific strategy: a way to manipulate tumor–immune interactions at the level where they are decided. By treating distribution and persistence as core biological parameters—rather than technicalities—this approach reframes therapy as the design of an immune event in space and time. In doing so, it aligns oncology with a broader principle of modern biomedicine: outcomes are rarely dictated by molecules alone, but by the systems they perturb and the contexts in which those perturbations occur.