In cancer medicine, there’s a persistent paradox: the most obvious target is often the hardest to control. A solid tumor is visible on scans, reachable by needles and catheters, and measurable in size—yet it can behave like a hub in a distributed network. Treat one lesion and the disease may still progress elsewhere. Treat the whole body and toxicity can become the limiting factor long before biology runs out of clever ways to adapt.
That tension—between local control and systemic disease—is the intellectual territory where AbscoTx lives.
This post is written to be safe and accurate. It sticks to broadly established scientific ideas and does not make claims about unpublished data, undisclosed pipelines, or timelines. Think of it as a “clean-room” explanation of the logic behind a modern intratumoral and immune-activating approach: why it exists, what scientific traditions it draws from, and why the concept is attracting attention across biotech.
The company focus: local delivery designed to matter systemically
Many next-generation cancer strategies share a common instinct: start exactly where the tumor is, interact with the tumor microenvironment directly, and try to create an immune response robust enough to recognize related disease elsewhere.
Intratumoral approaches (meaning the therapy is delivered into a tumor) aim to do three things at once:
- Concentrate therapy at the site of disease.
This can reduce the need for high systemic exposure, which is often where side effects emerge. - Alter the tumor microenvironment.
Tumors aren’t just cancer cells. They’re ecosystems—immune cells, fibroblasts, blood vessels, extracellular matrix, signaling molecules—sometimes arranged in a way that blocks immune attack. - Engage the immune system using real tumor context.
When local treatment causes tumor cells to die in certain ways, they can release antigens and danger signals that help the immune system “learn” what to target.
In the best-case story—one that scientists pursue carefully and skeptically—local treatment doesn’t stay local in its consequences. That leads us to a term you’ll see often in the intratumoral world:
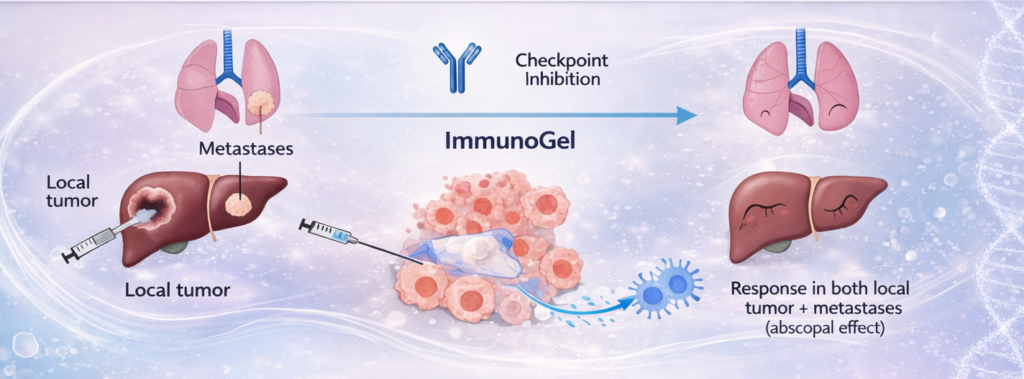
Abscopal effect: a phenomenon where treating one tumor site is associated with regression of tumors at distant, untreated sites. It’s not guaranteed, and it’s not a magic spell. But it’s a real enough concept that it has shaped a lot of thinking about how local therapies might “broadcast” immune information to the rest of the body.
A platform built around this idea is essentially asking: Can we make local delivery precise enough, durable enough, and immunologically meaningful enough that the immune system carries the signal beyond the injected lesion?
Why delivery matters: biology is picky about geometry
In biotech, it’s tempting to talk as if drugs are the whole story. In reality, delivery is often the story—especially in solid tumors.
A therapy can be potent in a dish and disappointing in tissue because tumors create practical problems:
- Uneven distribution. Some regions are well perfused; others are hypoxic or dense with matrix.
- High interstitial pressure. Tumors can push fluids outward, resisting penetration.
- Rapid clearance or leakage. If a drug diffuses away quickly, local exposure may be too brief.
- Immunologic “coldness.” Even if immune cells exist nearby, they may be suppressed or excluded.
This is where formulation science and materials science can become strategic. It’s not just “put drug in tumor.” It’s “place it, keep it there long enough, and shape its release profile to match the biology you’re trying to trigger.”
You can think of modern intratumoral delivery as an attempt to engineer time and space:
- Space: where the therapy goes (and where it doesn’t).
- Time: how long it stays, and at what rate it becomes available.
A platform approach—rather than a single molecule—often means the “product” includes not only what’s delivered (a payload) but also how it’s delivered (a delivery matrix, depot, or system).
A quick history lesson: from “poisons” to precision systems
The history of cancer therapeutics is, in part, a history of learning to control collateral damage.
The early era: cytotoxic chemotherapy
Many classic chemotherapies emerged from the observation that rapidly dividing cells can be selectively harmed—selectively, but not perfectly. These agents can be life-saving. They also illustrate a core constraint: systemic exposure tends to punish healthy tissues that divide frequently (bone marrow, GI tract, hair follicles).
The targeting era: small molecules and antibodies
Over time, oncology moved into more targeted strategies:
- Small-molecule inhibitors that block specific signaling pathways.
- Monoclonal antibodies that recognize cell-surface markers or ligands.
- Antibody-drug conjugates that bring a cytotoxic payload to a chosen target.
These advances improved specificity in many settings, but solid tumors are still heterogeneous and adaptive. Even precise drugs can face resistance, incomplete penetration, or immune evasion.
The immunotherapy era: checkpoint blockade and beyond
Checkpoint inhibitors reframed cancer therapy by unmasking the immune response rather than directly attacking tumor cells. For some cancers and some patients, the results are dramatic. For others, tumors remain resistant—often because the tumor microenvironment actively suppresses immune activation or excludes immune cells.
This is one reason intratumoral immunotherapy became interesting: you can treat the immune problem where it is being enforced. Instead of hoping a systemic immune modulator reaches the right niche at the right concentration, you engineer the niche directly.
Chemistry and “the depot idea”: why materials show up in biotech
If you zoom out, a lot of biotech progress is quietly driven by chemistry that isn’t glamorous but is foundational: polymers, excipients, buffers, stability enhancers, and controlled-release systems.
Controlled release isn’t new. In other areas of medicine, drug depots (long-acting formulations) have been used to:
- reduce dosing frequency,
- stabilize exposure,
- avoid peaks and troughs,
- improve adherence.
In cancer, the stakes are different because the target tissue is dynamic, hostile, and often anatomically complex. Still, the concept holds: if you can create a localized depot that behaves predictably, you can potentially:
- increase local exposure without increasing systemic exposure,
- sustain immune stimulation over a biologically meaningful window,
- reduce procedural burden by limiting repeated injections.
A “thermoresponsive” material, for example, is a class of formulation that can change behavior with temperature—liquid during injection, more structured afterward—so it can be placed by a clinician and then remain where it’s needed. The exact chemistry can vary widely (and companies often keep details proprietary), but the principle is straightforward: formulation becomes an enabling technology, not an afterthought.
This is a subtle but important shift in biotech identity. A company can be “a therapeutics company” even if its core advantage is a delivery system—because delivery can be the difference between an idea that works on paper and one that works in patients.
The biotech logic: platform thinking and modular payloads
One thing you see more often in modern biotech is the platform model. Instead of betting everything on a single drug, companies build a repeatable method for generating candidates or delivering interventions.
A platform intratumoral approach can be conceptually modular:
- A delivery system that places and retains a payload locally.
- A payload class (or several) that can be swapped based on indication.
- An image-guided clinical workflow that standardizes how therapy is administered.
When platform thinking is done well, it doesn’t mean “one-size-fits-all.” It means “one set of physics and logistics that can be applied across multiple biological contexts,” with each context still requiring real validation.
This is especially relevant in intratumoral therapy because tumors differ by location, vascularity, and accessibility. A real-world platform must respect clinical reality: what clinicians can inject, where, and how safely.
A cautious word about abscopal ambition
The abscopal effect is a powerful idea, but it’s also a word that can be misused. It doesn’t mean “inject once and cure metastasis.” It means something more nuanced:
- A local intervention can, under some conditions, create systemic immune consequences.
- Those consequences may vary by tumor type, patient immune status, and therapy combination.
- Reproducibility is the hard part—turning an observed phenomenon into a reliable therapeutic strategy.
A responsible company in this space tends to talk about abscopal effects with disciplined language: as a goal, a hypothesis, a direction—not as a guarantee.
That discipline matters because cancer is not short on inspiring stories; it’s short on interventions that hold up under broad, repeatable clinical testing.
Where this all points: a modern synthesis
The most interesting biotech companies often sit at the intersection of disciplines that used to be separate:
- Immunology (how to activate, steer, or unmask immune attack)
- Oncology (tumor heterogeneity, microenvironment, resistance)
- Chemistry and materials (how to control release and localization)
- Clinical workflow (what is feasible, repeatable, and safe in practice)
- Imaging and intervention (how to place therapy precisely and confirm placement)
An intratumoral delivery platform motivated by abscopal thinking is essentially a synthesis of those areas. It’s a bet that precision placement + controlled exposure + immune relevance can unlock better outcomes than systemic therapy alone in certain settings.
It’s also a bet that the “last mile” of therapy—how and where it’s delivered—can be engineered as carefully as the drug itself.
Conclusion: a simple north star
At the heart of this kind of company is a simple north star:
Make local treatment precise and durable enough that it changes the systemic conversation between tumor and immune system.
The science behind that goal is real, but it’s also demanding. It requires careful attention to delivery physics, immune biology, and clinical practicality. It requires speaking in hypotheses rather than hype. And it requires proving, step by step, that a local intervention can produce meaningful systemic benefit without unacceptable trade-offs.
That’s the kind of biotech story that ages well: not because it promises miracles, but because it respects how hard biology is—and still insists that engineering, chemistry, and immunology can be combined to make better tools.
In a field where “breakthrough” is a word that gets tossed around like confetti, the more durable excitement comes from something quieter: a platform built on first principles, tested like reality matters, and designed to translate from lab logic into clinical practice.